
About the event
Imperial College School of Medicine Endocrinology Society is excited to present to you our annual online conference in 2021!
About this Event
Join our conference to learn more about inspiring topics in endocrinology in the 21st century from leading researchers and clinicians in this field. We are extremely honoured to host speakers from the universities of Bristol, Queen Mary University of London, St George’s University Hospital and our own Imperial College London. They will be presenting an exciting range of topics from endocrine signalling in paediatrics and 24-hour hormone profiling during working days, to endocrinology in transgender medicine and interesting cases from clinical practice. Our conference will present you with a fantastic variety of talks which will enrich your endocrinology knowledge and give you a new perspective on what a career in this field might look like.
We look forward to welcoming everyone on Saturday 13th February! All are welcome!
Blurb from Eventbrite
There had been a whole day of talks given by consultant endocrinologists to undergraduate medical students in the UK and all over the world. The last agenda item of the day was with Dr Leighton Seal, Consultant Endocrinologist, St George’s Hospital, who works with the Gender Identity Service at the Tavistock (he made a point of saying this even though his profile lists him at Charing Cross) and also provides private hormone management to transgender patients with Gender Care. The topic of the item was ‘Gender Identity Medicine’.
Opening gambit
Dr Seal started by explaining that one of the causes of gender confusion could be because someone might be ‘intersex’ (i.e. a Disorder of Sexual Development – DSD) and that this is one of the main things which would be investigated at a gender identity clinic.
Understanding of terminology was also going to be important in order to deliver ‘respectful’ care to gender dysphoric patients.
Finally, hormonal treatments would be discussed, including risks and benefits, and surgical treatments.
Big caveat from me
Dr Seal referred to the ‘two genders’ and not to biological sex, I will however refer to sex. For clarification I am not a medical person so I have no idea how accurate Dr Seal’s presentation was. Clearly some of it was bollocks though.
Embryonic development
Dr Seal outlined how the embryo develops and explained that if an embryo with XY chromosomes if there was a failure in the production of testosterone then normal sexual reproductive development would not follow. He then claimed that the process continued ‘post-natally’ and showed us a photo of a child and said we would not know if the child was male or female but that we could not do that with an adult. Hmm. Interesting example to compare a pre-pubertal child with an adult.
Differences in male and female brains was driven by pre-natal androgen exposure, resulting in differences in the hypothalamus (males have a bi-annual cycle, females roughly 13 cycles per year). A number of brain structures were different in size between the two sexes.
Within those different structures there were hormonal receptors and during high aromatase activity (i.e. oestrogen producing cells) testosterone was converted to oestrogen.
Dr Seal told us that by 5/6 weeks a male embryo would be producing adult male testosterone levels and after birth a baby boy would continue to a second peak of adult male testosterone levels. Differentiation of the gonads was complete by 12 weeks in gestation with brain differentiation happening between 15-24 weeks. Therefore, Dr Seal argued, there may be enough testosterone to cause differentiation of the body but not enough to cause cerebral differentiation and ergo female ‘somatic’ development. (He was basically inferring this was the cause for a transgender brain in males.)
The difference between sexual orientation and gender identity
The two things were completely different and Dr Seal said:
I’m male. I’m happy being male, I’m settled as male. I could equally well be a male who wants to have sex with men, or a male who wants to have sex with women. But my masculinity, my male gender identity, is separate to sexual orientation.
Dr ‘I’m male’ Seal, with a male gender identity
Dr Seal then went into various DSDs and said that these could give ‘strong clues’ on how genetics and hormone production and gender identity interacted. Complete Androgen Insensitivity Syndrome (CAIS), Seal said, resulted in ‘strongly feminine gender identities’. Congenital adrenal hyperplasia (CAH) he felt was a far more interesting condition and said that toy choices of females affected by CAH were not to play with ‘girls’ toys’ but with ‘boys’ toys’. The control in the experiment were provided by ‘unaffected siblings’ (irony overload). In adulthood CAH females were more likely to be homosexual and had poorer maternal instincts. Dr Seal said that antenatal androgen exposure had changed their behaviour.
Brain specimens
Then Dr Seal put up a slide of the supposed differences between the brains of three different types of men and one woman. It’s all very sciencey, innit?
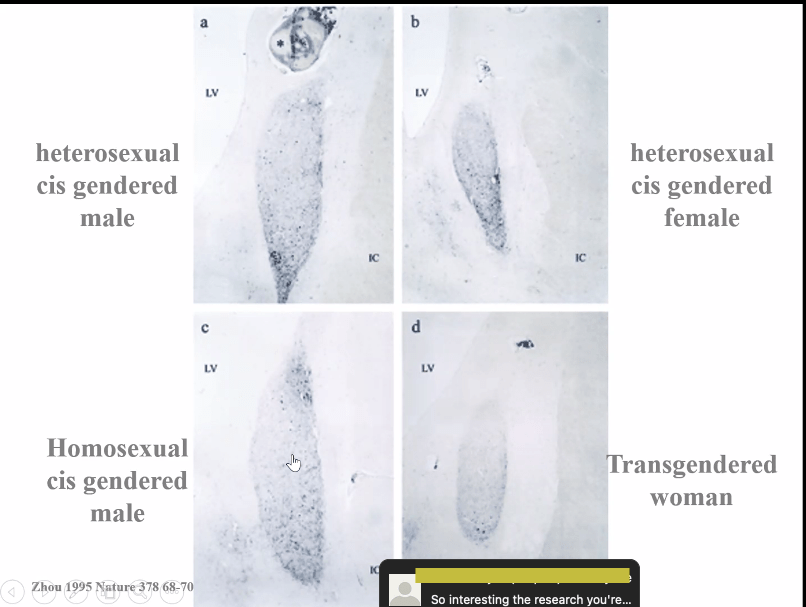
Do you want to know which part of the brain you’re actually looking at? So would I. Dr Seal referred to them as ‘cerebral structures’. There was no difference between A and C Dr Seal said, but just look at how similar B and D were! Actual lady brains!
They have such a strong female identity that they present for treatment. I think you can see unequivocally, whatever is happening below the neck, above the neck this person has female structures.
Dr Leighton Seal, talking shit
Dr Seal’s role in the gender identity clinic
Firstly he assesses patients to find out if they have a DSD and secondly he monitors and supervises the hormonal treatment. The commonest condition he sees is CAH and the incidence of this was one in a thousand. Which is very interesting because in his NHS profile at St George’s Hospital it does not mention that he treats patients with DSDs at all, but rather thyroid disorders and erectile dysfunction. They must all be turning up at his gender identity clinics then.
Differences between trans women and trans men
Dr Seal was really on the tightrope explaining that men typically decided to transition much later than women and that in the adult clinic there were twice as many men as there were women. (Wonder how the brain differences account for that then?) In the adolescent clinic however, it was two to one of females over males. Over time these ratios looked to be levelling out. Also in Japan there have always been many more women who have transitioned over men.
The all important terminology
Dr Seal said he had no interest, as a doctor, in people who were gender non-conforming but was interested when society ‘had imposed ideas of gender on a person and then that causes distress’ which was known as gender dysphoria. So, not anything to do with the brain or embryonic development then. Phew!
Non-binary genders included people who have a mix of genders or no gender at all and there were currently 35-30 separate terms that non-binary people used to describe themselves. Ask them how they define themselves and ask their pronouns! advised Dr Seal – sadly we didn’t get to hear about the genetic or medical reasons for non-binary genders.
Gender incongruence and the ICD 11
Previously gender dysphoria had appeared in the International Classification of Diseases (ICD) in the mental health section. However, in the latest release of the ICD (no. 11), it would become ‘gender incongruence‘ and would be under the sub-category of sexual health. Dr Seal summarised gender incongruence as there being ‘a marked incongruence between one’s felt gender and the gender other people would impose upon you’ and that to have this diagnosis meant you did not have to have any significant psychological distress.
Hormone therapies
When we talk about hormone therapies the principle of treatment is triadic. We try to have progressively more interventional treatments that are harder to reverse.
Dr Seal, sounding sinister
The first stage of treatment is to have the person transition socially, i.e. changing name, having preferred pronouns and dressing differently, this has the bigger psychological impact over anything hormones could do.
Then comes the hormonal therapy which should produce the secondary sex characteristics of the target gender.
After a year of both social transition and hormones then surgical approaches might be used to alleviate the gender dysphoria further (which will no longer be a psychological problem as of 1 January 2022 when the ICD 11 is adopted). However, bilateral mastectomy could be considered after only six months, because it was very difficult to occupy a male gender role with breasts. Okay, so it’s six months then.
Screening tests
Hormone testing was done to see if there were any issues with hormone production to see if there were any of the intersex conditions present, however karyotyping to look at the genotype was not generally done.
Gender dysphoria has never been associated with karyotype abnormalities.
Dr Seal, contradicting himself
In fact as Dr Seal continued, it appears that the hormone testing screening is needed to ensure that it was safe to start the patient on the dangerous cross sex hormones which would clash with their patient’s own endocrinological system, especially for those who might be diabetic. Cardiovascular risk was the biggest concern though, which means that blood pressure needs to be monitored.
Treatment for men
Aim of therapy
Firstly suppress the genetic sex hormone production, then induce the secondary sex characteristics of the opposite sex, and finally, after gonad removal, therapy is needed to prevent hypogonadism (Dr Seal did not explain what this might entail).
Dr Seal spoke about the changes to a man’s body on oestrogen. The average breast growth a man could expect was the average for the British population – a B cup.
Greater doses of hormones did not result in more changes and genetics plays a big part in the kind of changes one might see (basically your doctor will not be able to tell you what will happen so you could be left with minimal or gross cosmetic change, either way the bone thinning is real).
Anti-androgen therapy
Men on oestrogen also need to take drugs in order to suppress their androgen production, this is normally with spironolactone, however this can compromise ‘breast development’ and they get ‘stuck’ between Tanner Stage 3 and 4, which was demonstrated with photos of normal pubertal breast development on a girl (clearly a man’s breast development would have been more instructive).
Another drug which could suppress androgen was a GnRH analog called Decapeptyl (normally used to treat prostate cancer). Decapeptyl overstimulates the hypothalamus which then shuts down the production of testosterone altogether. This results in chemical castration which would result in an identical profile to that of a man who had been castrated.
Despite giving men more than five times the dose of oestrogen than would be given to women on HRT, many men still could not achieve an oestrogen level in the target range. It is thought this is because the liver is metabolising the oestrogen and stopping its release into the body. In that scenario topical oestrogen would be started. Dr Seal referred to oestrogen taking in men as HRT.
Complications of therapy
Dr Seal made much of the impact of smoking on patients taking cross sex hormones. The biggest risks were thromboembolism, strokes and raised prolactin. Dr Seal said that 90 percent of transgendered people had Vitamin D deficiency and inferred that this was a problem present prior to hormone therapy (might it be that people have already started black market therapy before turning up in the gender clinic?). Therefore Vitamin D replacement was given.
Dr Seal boasted that in the UK only GnRH analog therapies were used to suppress androgen production and that they had fewer side effects. American health insurance companies would not pay out on them because they were expensive.
Lifelong treatment
Men on oestrogen can stay on the treatment lifelong. Women who take HRT to treat menopause symptoms are taken off it routinely around aged 55.
Men with breast development are advised to join the mammography screening programme aged 50 onwards and also need aortic aneurysm screening.
Surgical intervention for men
Dr Seal showed a series of graphic photographs of a vaginoplasty being performed on a man.
First of all we take a skin graft from the back of the scrotum, which will be used to make part of the vagina. Then you fillet the penis and remove the penile skin. You remove the testes. Then you take a nick out of the glans penis, preserving the neurovascular bundle, this will form the neo clitoris. Then you bury a hole between the rectum and the bladder in the front, which will form the vaginal cavity. You make a hole for the clitoris and a hole for the urethra. Then you sew the scrotal graft onto the penile skin and you invert things. Six weeks later this is the cosmetic result*.
Dr Seal
*Not entirely sure that the final after photo was of the same person in the before photos. However, if it was, it was an amazing cosmetic result, and nothing like you-know-who’s new undercarriage.
Treatment for women
One of the first changes you see are changes in genitalia, so enlargement of the clitoris and cessation of menses. The skin becomes oily which is a recognised side effect of testosterone. They also get atrophy of the vaginal lining, so they go into a menopausal state, as far as the genital tract is concerned, as oestrogen is no longer being produced. […] If they are programmed to go bald, unfortunately that will happen.
Dr Seal
Dr Seal also referred to testosterone treatment for women as hormone replacement therapy. Women are given the same doses that are given to men in the normal HRT setting. Sustanon is licensed to be used to be given to women, Dr Seal said. The information page I have linked clearly states the ‘safety and efficacy of this medicine has not been adequately determined’ in children and teenagers and gynaecomastia (breast tissue formation) is a known side effect. Dr Seal didn’t clarify the age groups he thought Sustanon might be suitable for.
Pregnancy
Dr Seal talked about pregnancy risks and warned the medical student audience not to assume that ‘transmasculine’ persons were not attracted to men and said there were many gay trans men out there. At the moment he was supervising three people who are actively having a child at the moment (one wonders what kind of supervision, since his speciality is not obstetrics).
Always discuss reproductive options with people before they start treatment. Get some idea of what their idea of parenting is, and whether they would like to use their own genetic material. Also whether they would like to carry the child themselves.
Dr Seal
Side effects of testosterone
Dr Seal said that testosterone was generally safe to use in female patients and that although the myocardial infarction rate was higher than for women who did not take testosterone, it was lower than the male population (again, one wonders how such a statistic was compiled). Haemocrit (raised red cell levels) and raised lipids however were significant worries. Dr Seal didn’t expand on any of the associated risks that these two blood profiles might provoke or any long term effects.
Dr Seal explained that testosterone could sometimes be converted to oestrogen via aromatase enzymes and therefore such women needed to present themselves for ultrasound scans to ensure that the lining of the womb was not thickened. One study suggested that about 15% of women on testosterone would develop this complication. Dr Seal said that he felt that it was a ‘dramatic overestimation’.
Dr Seal said that overall studies suggested that bone health is maintained on testosterone therapy.
Aim of therapy
The aim of therapy was to keep testosterone in the male range for as much of the time as possible. Injections had a peak effect where the testosterone might go higher than the normal male range. Therefore tests had to be done the week before an injection and a week after an injection. With gels and long acting injectable testosterone the testosterone level was kept in the middle of the male range; ‘because we know then that testosterone for most of the time will be okay’. Not exactly reassuring.
After ‘things’ were stabilised it would just be ‘an annual review of the blood tests that we would do’. Like really? Are you fucking serious? Even women on the oral contraceptive pill have quarterly reviews and that’s a microgram dose.
Other issues for women on testosterone
They should be part of the national cervical smear programme. After bilateral mastectomy the risk of breast cancer is massively reduced but it was not zero and it was still advised that they do regular breast checks on themselves.
Surgical intervention for women
Dr Seal showed the students graphic photo details of a phalloplasty being performed and described the surgery in detail. Basically skin is taken from the thigh or forearm and is rolled up to make a neo phallus (‘like a double sausage roll’), including a catheter. Testicular implants would also be added. An erectile device might also be inserted so an erection could be achieved.
Dr Seal then showed us a photograph of a woman who had had a metoidioplasty. This is an easier procedure to have and had fewer complications. The clitoris was ‘released so that it can enlarge’. The urethral opening is moved up towards the end of the clitoris and skin grafts from the mouth are often used.
Dr Seal said that most trans-identified females wanted to be able to pee standing up and that penetrative sex was a secondary consideration for them.
The photo of a metoidioplasty itself was one of the worst things I’ve seen. The woman had a phallus which looked like it belonged to a prepubertal male but it obviously had the darkened colour you expect to see in an adult woman. The tiny testicular implants worsened the cosmetic effect considerably.
What about the non-binaries?
Well quite. Why would they need treatment?
Dr Seal told the medical students that it was very important to have very clear ideas about what the results of hormone would be with non-binary patients. The input from the psychiatrist/psychologist was particularly important. Was the person’s sense of identity fixed or fluid? Is there a clear idea of what mix of male and female features the person wants? Psychological co-morbidities were very important.
Hormone therapy could be standard or there could be a mix and match approach to achieve their specific goals. For those non-binary people who did not want any secondary sexual characteristics from either sex (i.e. complete androgyny), a ‘neutralising’ therapy would be used instead. Talk about experimental.
A woman with a non-binary identity who wanted a beard but did not want enlarged genitalia – well that wasn’t really possible with testosterone. However, a man who wanted breast development but low impact on sexual functioning, well that might be feasible with the various oestrogen products available.
Long term outcomes for patients with gender dysphoria
It was known that patients who were trans-identified had an increased mortality risk. A Swedish study showed this was due to suicide and substance misuse but also an increased risk of cardiovascular events. Dr Seal blethered about the axis or something or other and came to the conclusion that:
In summary, Sweden was quite a nasty place to live as a trans person previously, because people were dying of suicide, but now with this becoming better, it looks like it is getting better to live there.
Dr Seal
A Holland study, which looked at outcomes over 17 years, showed increased risks of suicide, substance abuse, ischaemic heart disease, and HIV acquisition. Again Dr Seal minimised what the study showed citing improvement in drug regimes and societal changes.
Dr Seal told the medical students that as long as patients were monitored on hormonal therapies they were safe and effective and provided psychological relief.
Question and Answer session
The two students hosting the Society’s event were very clear that this had been their favourite session and that this topic was not included in the curriculum normally.
What counts as girls toys and what counts as boys toys and are these not culturally influenced?
Dr Seal totally accepted that these were cultural constructs and explained that the experiment was set up around these constructs. He admitted that the study he used was from the 1980s. Dr Seal said that very young children would still try to stick with their peer group, thereby confirming that many kids will simply conform to expectation and some won’t.
How do you support trans men who chose to become pregnant? Is it as simple as stopping testosterone therapy?
There was very limited knowledge about this but there was one study ongoing. Dr Seal said that patients were encouraged to preserve their fertility prior to commencement of hormone therapy. Becoming pregnant with your own genetic material was simply a case of stopping testosterone and over the next six months 60 percent of women returned to normal menses, within another year 95 percent would return to normal menses. A testosterone check should be performed prior to attempt of pregnancy. Dr Seal claimed that all the babies which had been born from women ‘in that way’ had all been healthy. He currently had ‘three on the go’, a trans man who was married to the same trans man he had helped the previous year, a non-binary person and a trans guy who was trying to get pregnant.
The real impact on women in these circumstances wasn’t the mix of hormones swilling about in their systems, but the psychological impact of being perceived as female. Delivery rooms were very ‘gendered’ environments. Use parent, rather than mother. Reduce the number of triggers for that person and validate their gender identity. ‘That’s a he/him person who is having a baby,’ said Dr Seal. ‘That’s so interesting,’ said the student who had organised the conference, ‘thank you so much’.
Has surgical intervention increased over the last decade?
The clinic had increased in size every five years over the last decade. The percentage of surgeries had not increased but the numbers had gone up.
You showed a slide which showed histological sections from brains from cis- and trans-gendered people in the beginning. Would you mind repeating your statement?
So those were post-mortum slides. So they’re people who have died – what an unfortunate name – there’s a guy called Dick Swab, in Holland, who has a brain bank. So he has bank of brains that he has just collected over the years. And within that brain bank he had people that were treated for gender dysphoria, their [sic] had people who were cis as well. In the- in the- specimens he had men treated with oestrogen for prostate cancer, so in the old days we used to use oestrogen to treat prostate cancer, because we didn’t have GnRH analogs. Those men had male brains, whereas we have got trans women who have female brains. It doesn’t therefore appear to be the oestrogen itself which is causing the changes to the brain structures, it seems to be something intrinsic to the brains of those people.
We even had a trans woman who declared herself as trans but had never been treated, so- but she was too old to be treated, but she felt that at the time that she died, she had a female brain, even though [she] never been exposed to oestrogen whatsoever.
So it appears that there is some biology behind this somewhere.
Dr Seal, clearing things up
On queer brains
Then a student wanted to ask a question herself personally. She thanked Dr Seal and asked if she could have a copy of his slide presentation. She thought the work was important and that medics should be educated in this area. She wanted to work with him. She asked him about the ‘queer brain’. Dr Seal said that sexual orientation was difficult to define and quoted Kinsey material and the Kinsey Scale and appeared to suggest that most people were bisexual really. Dr Seal was concerned that conversations about the aetiology of homosexuality or transness might result in people trying to cure it.
The student agreed with Dr Seal and said that there was a danger of medicalising the patient because of their identity. She wanted to know about how the psychological therapy worked in tandem with hormonal therapy. Dr Seal said that he worked as part of a multidisciplinary team and did not take direct referrals. The team was made up of endocrinologists, psychologists, psychiatrists, speech and language therapists, they also had an oncologist who was training in gender, sexual health medicine, GPs and primary care specialists. Patients saw improved levels of depression and anxiety. Dr Seal said that no one in the field believed that gender dysphoria was a psychiatric disorder:
… however, transition is terrible, still in modern society to be a trans person is a bloody awful thing, especially this year there has been open transphobia in the media.
Dr Seal
Dr Seal continued contradicting himself, yes trans people experience mental distress, but not because they’re trans. Transition might also result in loss, like losing a partner or job. Psychological resilience was needed to tolerate transition.
So basically people are assessed either once or twice before to make a diagnostic assessment and then if hormone therapy is appropriate, then hormone therapy is put in at that point.
Dr Seal
How many non-binary people did Dr Seal treat currently? What specific barriers did they face compared to binary trans people?
Dr Seal said the current caseload of patients was about five thousand of which ten percent were non-binary and that this was going up all the time. Dr Seal that the psychiatrists and psychologists managed the hormones in routine cases, and that a case would only come to him if it was complex. All non-binary patients were being reviewed in the endocrine clinic because they needed tailored treatment plans. In a week he might see 6-7 people with a non-binary identity.
Access to healthcare was more difficult for them because a lot of people didn’t understand it, including the GP who would be responsible for making the initial referral. Dr Seal advised the medical students to take extra time to find out what pronouns they would like to use. Non-binary people had it worse because they will have to undo everyone’s assumptions. In the past non-binary people were lying to clinics about their identity, for example a woman in the past who simply wanted mastectomy might have taken testosterone in order to gain access to the surgery. Being open about being non-binary meant that surgery could be pursued alone.
The clinic employed medical professionals and admin staff who identified as non-binary.
Do you consider genetic disposition to play an essential role for transgender people?
Dr Seal pretended not to understand the question. Some behaviours were intrinsic and the endocrine system was probably the best example of this, for example in traditional society women do not tell people that they are pregnant until the first 12 weeks are over, and this was a socialised behaviour driven through hormones. Then Dr Seal gave all examples of children behaving in ways which was against sex stereotypes as proof that the ‘transness’ had been present all along.
Plug
Dr Seal is the clinical director of the Royal College of Physicians Gender Identity healthcare programme. The programme was for post-grads, registrar level and above, but he urged the medical students to sign up. It was a 2-year MsC diploma course in Gender Identity Healthcare. It was launched in 2020. The Royal College of GPs also had a training programme which was ‘quite good’.
Dr Seal was right about one thing though, Dick Swab is an unfortunate name.
Thank you for reading! Sign up to my blog by going to the bottom of the page.
Please share on other forums if you liked it, as I only do Twitter.

I don’t know about HRT for women ending around 55. You can start it any time during the menopause and stay with it as long as the symptoms last.
(I didn’t start till last year and I’m past that age.)
Depressing read, though. I don’t know how you sat through those images.
LikeLike
Dear me,
i may manage the whole article at some point but gave up as damn that is some muddled shite! :(!
Thank you for documenting, incredible attention and patient! effort.
That guy should not be lecturing or in practice. ….. Damn 😦
How is this happening in the 21st century?
What happened to stds? Why does no one in the profession call out bilge?
What about the patients?
Hope he has very few.
LikeLiked by 2 people