
A thorough and inspiring discussion on the healthcare needs of trans people.

What do we mean by ‘Inclusion, Good and Best Practice’ discussions, talks, recommendations, community voice.
Trans Health Matters is a series of conferences by CliniQ CIC Holistic Wellbeing, Sexual Health and HIV.
This event is delivered in partnership with King’s College Hospital NHS Foundation Trust
Our aim is to advance and share best practice and to continue to build and develop services for trans and non-binary people that are inclusive, respect diversity and address health inequalities.
The event is for clinicians, commissioners, policy makers, community organisations, the voluntary sector and for trans, non-binary and gender diverse people.
We will have a strong rights and equalities focus and will look at specific health needs and issues surrounding trans and non-binary people’s inclusion in the planning and delivery of health and social care services, with a view to reducing barriers to services and moving towards an inclusive approach to trans health matters.
From the blurb on Eventbrite
Programme:
13:10 – 13:30
Keynote: Inclusion Matters.
Rico Jacob Chace (He/Him) Director at TransActual UK, Trustee at LGBT+ Consortium, Diversity & Inclusion Consultant.
TransActual UK are a relatively new organisation having been set up in June 2020 as a Community Interest Company. Rico Jacob Chace, a trans-identified female is a diversity consultant and available for hire.
Chace told us that CliniQ is now ten years old and is also a Community Interest Company. It is the only gender identity service in the UK which also offers holistic services, including yoga and self-esteem building events. It raises funds for itself by offering training programmes and conferences, rather than direct funding from the NHS, however it is partnered with King’s College Hospital, who I expect funds most of its activities.
Chace was very keen to bring attention to Michelle Ross, very much the driving power behind the entire project, but Ross demurely batted away any such attention with the flutter of hands and batter of eyelashes.
Because ‘transphobia’ was on the rise it was becoming increasingly difficult for people to talk to their GPs about their healthcare needs (and when they say ‘healthcare’ they really mean access to cross sex hormones). Thus began the conference which repeatedly focussed on GPs having the responsibility to manage ‘trans healthcare’, which really requires the monitoring of an endocrinologist, if anyone was to be saddled with such a responsibility.
13:30 – 13:50
Understanding and addressing health inequalities for trans and non-binary people.
Dr Michael Brady. (he/him) National Adviser for LGBT Health, NHS England – followed by Q&A.
Dr Michael Brady is National Advisor for LGBT Health at NHS England and Consultant in Sexual Health and HIV at King’s. Brady gave a talk with slide show. ‘Transphobia’ was having an impact on the health of trans people, because a day wouldn’t go by without a negative article in the media and the arena of social media was particularly bad. Brady wasn’t able to give specific examples of health inequalities but did want to draw attention to mental health being much worse.
He had a three point action plan to improve things.
1. Monitoring and data collection
The LGBT Foundation had produced a document on monitoring (available here). In particular, Brady really really didn’t want two of the following slides to be shared publicly, no idea why since the data from the GP patient survey is publicly available to search here and will even generate specific reports. I have eyeballed the slides several times and can see nothing controversial about them. I expect a further breakdown of age and gender will reveal that males occupy the upper age scale, and females the lower.


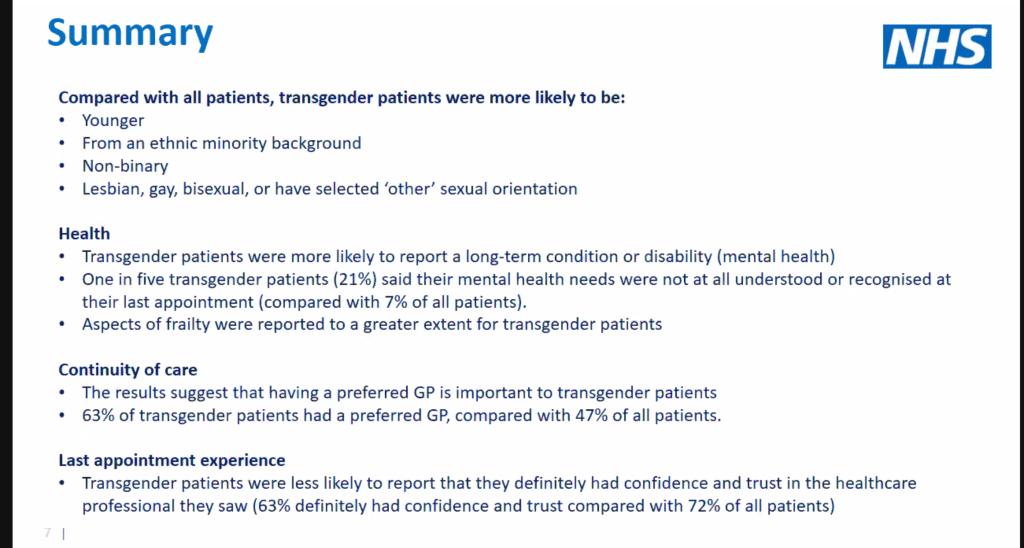
You will note that the new question in the GP Patient Survey has been worded in such a way that people are forced to comply with the idea that they have a gender identity, or else leave their sex as potentially unclassifiable if they choose ‘prefer not to say’. Similarly trans-identified people are encouraged to answer exactly how they like. Great data collection, innit?
2. Training
Dr Brady told us that hetero- and cis-normative culture needed to be challenged and that training should be informed and delivered by LGBT+ people. Allies could educate themselves. Indeed Brady had recently been doing his own education, reading a book by Juno Roche called Gender Explorers, which has a foreword written by Susie Green of Mermaids and an afterword written by Jay Stewart of Gendered Intelligence, and is specifically focussed on interviews with children. Brady told us the book gave him a ‘moist eye’.
3. Inclusive Services
As well as sticking Rainbow Flags everywhere, and having pronouns on display at all times, Dr Brady also wanted services to use non-gendered language, which isn’t exactly brilliant when many health conditions differ between the sexes (Dr Brady works in sexual health services so must understand this).
He felt the maternity services provided by Brighton and Sussex had done particularly sterling work in avoiding the use of the word ‘woman’ and posted this link as an example. He did not mention, of course, that most women who take testosterone induce infertility and often require hysterectomy, but remember this was a trans healthcare conference, so why bother mentioning that?
Q&A
There was excitement about what the 2021 Census Data may show in terms of the trans population. As per usual there was undue focus on clinic receptionists being the keystone for providing warm fuzzy gender feelz, not the first choice for most when looking for warm fuzzy feelz it has to be said, and certain proof they’re not really in touch with reality. In fact, CliniQ has developed a unique way of undermining their own reception team, by using a team of volunteer greeters in the reception area (a video later revealed how small this area is).
Making things happen relied on showing things were bad in the first place and it was reflected upon that getting the NHS to provide PrEP for free had been a joint effort of many voluntary organisations, charities (notably the Terrence Higgins Trust), and other activists. It had also involved court action.
By positioning CliniQ at King’s College Hospital this had put users front and centre – which is clever when you think about it – imagine if a Hospital Trust did that for their diabetes patients?
Michelle Ross told us all that there was no problem having more people round the table, you simply needed to get more chairs, which is a bit like when people talk about the pie of rights – that you can just ‘grow the pie’. An easy way of avoid difficult conversations about competing needs.
Dr Igi Moon, Chair of the Memorandum of Understanding against Conversion Therapy (i.e. the version of the conversion therapy ban which would criminalise therapists from talking through conflicts between sexuality and gender identity), basically asked a question so that she could announce her attendance, which was on the need for inclusive training across the NHS.
13:50 – 14:20
Sexual Health and HIV – What Needs to Change?
I was today old when I learnt that Public Health England has been split into two organisations, the UK Health Security Agency (UKHSA) and the much less sexy sounding Office for Health Improvement and Disparities. COVID 19 has surely put a rocket up everyone’s arse and health and security are now forever intertwined.
Sexually Transmitted Infections and Trans and Non binary people. A first update on data with a Principal Scientist
We were given a presentation by one of the principal scientists from the UKHSA, who told us her pronouns were she/her. The Agency has developed a new mandatory surveillance system for STIs and new data collection included condom use, recreational and sexualised drug use and outcomes of partner notification, plus people could also declare their gender identity (no acknowledgement made that such declarations will change over time).
We were told that trans people had had very little visibility in sexual health services historically – again no acknowledgment that numbers in the past were far fewer. Some trans people were at higher risk of STI than the rest of the population – I suspect these are sex workers, but no further information was given.

The UKHSA is recording sex and gender identity in the same sloppy manner as the GP Patient Survey, implying that gender identity is inherent and making it impossible to entirely disaggregate sex and gender identity, especially in the cases where people declare a ‘non-binary’ identity. You have one job to do! Collect data.
Provisional data collection suggested that about two-thirds of the transgender patients attending STI clinics were male.
HIV Reporting System- an update: example in good data collection.
A consultant epidemiologist, who also told us his pronouns, said that the data dictionary of the HIV reporting system had been updated to include trans and non-binary identities. The number of people being diagnosed with HIV was decreasing year on year and in 2020 there were just under 2,000 newly diagnosed patients, none of whom were ‘transgender’, but there were ‘about five’ who identified as ‘non-binary’. I suspect no one quite knows what this means.
Both sessions will be followed by a Q&A
Nope, no time for questions!
14:20 -14:35
‘HIV Made Me Fabulous’ is a 10-minute film that tells the personal story of Juno Roche, a writer, activist, and trans woman, who has been living with HIV for over 25 years.
We were shown this film written and narrated by Juno Roche. I have posted about this separately because I did go on about it rather a lot, which you can read here. Needless to say ‘HIV made me fabulous’ is a very poor public health message to share about a life long incurable and still deadly disease, which requires daily medication and regular monitoring, especially when many trans-identified people also embark on long term cross sex hormone use, which requires the same. Crackers. Watch it for the dancing.
14:35 – 14:50
Older Trans People Matters – King’s College Hospital and CliniQ our survey.
The Gerontology Department at King’s has launched a survey which seeks to find out more about the older population of trans-identified people and are asking that those in this category complete the survey if they are aged over 50. The data is completely anonymised and therefore won’t be reliable. They won’t be asking any questions about how cross sex hormones is affecting bone health and/or mobility, but might ask that at a later stage if they continue the project. Thus a completely wasted opportunity to find out or inform on any relevant clinical issues in the first instance. One suspects that this is because they don’t want to trigger their intended audience, but if that is the case, how will engagement be sustained long term if trepidation is the starting point?
The panel felt more comfortable discussing instead that the word ‘geriatric’ was stigmatising and that a new LGBT retirement community had been set up.
14:50 – 15:00
Comfort Break
Just time to put the kettle on and a hypocritical use of my own gender neutral loo!
15:00 – 15:15
Community Voices Victoria Gigante and Victoria Cordoba.
Victoria Gigante is a member of the Stonewall Trans Advisory Group and a greeter at CliniQ. He explained to us that when people arrive in the clinic he offers hand sanitiser and a mask. Never a dull day, eh?
Victoria Cordoba is also a greeter but relatively new. He spoke about the new mentoring scheme that was being rolled out for people on CliniQ’s counselling waitlist. Volunteers would be responsible for providing the mentoring, which would include advice on how to manage stress – but really it just sounded like grooming to me. Surely it would have been much more productive to hire an extra counsellor to get the waiting list down, than to send four people on a four day training course (which in turn now makes me wonder who provided that training and was this a self-fulfilling endeavour for CliniQ as a company). No ‘trans masc’ or ‘non binary’ person received training, which is entirely unsurprising and further proof that diversity mantras are purely that.
The mentoring service was for those over 18 only, and trans activist Octavian Star was keen to establish if teenagers could register for the service before their 18th birthday.
15:15 – 15:40
Cervical Screening Trans and Non binary people Video: Speaker Octavian Star with Q&A
We were shown this short video about going for a cervical screening appointment at CliniQ. To be fair, in comparison with other videos educating trans-identified females on the same, this is one is actually not that bad. It’s a highly competitive field. Hilariously we see that volunteer greeters do nothing more than walk people two metres to the receptionist.
Women who take testosterone have a vastly different clinical picture to women who don’t. That is not explained at all, and the problems are summarised below, though the most important point is that testosterone causes muscle atrophy, meaning that the womb and vagina vault shrink, with the cervix ending up in a different position.

Octavian spoke after the video and told us that she no longer requires cervical screening because she has had gender confirmation surgery – so the perfect person to front the video published only a few days earlier! We were told that once you are recorded as a male at your GP surgery, reminders to attend cervical screenings would no longer be automatically generated. There was much consternation that reminders would then have to be manually created or that women would be not be called at all.
A nurse practitioner from CliniQ who performs cervical screenings, and whose pronouns were she/they, told us some factual information about cervical screening protocols, however she/they wasn’t able to answer questions about colposcopies, or if testosterone use increased the risk of cancer. Brilliant, really knowledgable.
Women who had had ‘gender confirmation surgery’ might find it particularly embarrassing to have a cervical smear (funny how one is embarrassing but the other life affirming – either way its exposing your genitals).
Stewart O’Callaghan, the founder of Live Through This, a charity linked to Maggie’s Cancer Centre at Barts Hospital, London, had been due to give a presentation at the meeting, but couldn’t make it. He has they/them pronouns, and 3 out of 4 members of the team identify as transgender. The fourth one, who identifies as an ally, is Dr Alison May Berner, part-time medical oncologist at Barts and part-time specialist registrar in gender identity at the Tavistock. Mind blown.
Dr Ally Cat (geddit), as she is known on Twitter, has co-written an article with O’Callaghan on Understanding the role of sex hormones in cancer for the transgender community, I followed the link on the Queering Cancer Instagram account but found no link to the paper, however there is an admission that the ‘researchers found that hormone therapy may increase the risk of certain cancers’. So that’s okay then.

Live Through This will be launching an awareness campaign to tie-in with a national campaign day. They would be producing further videos next month and had been the producers of the My Cervix My Service video.
I wonder what difference these videos ever make and what is the point of producing more of them?
15:40 – 16:10
Panel Discussion – Why are Local Services Needed for trans and gender diverse people? 3rd Sector, Community, NGO’s working with NHS. What needs to change? How do we implement the inclusion in all health service in partnership with community and NHS…
Not a panel discussion at all. People merely introduced themselves, and in some cases for a second time.
One told us that trans people had to wait two years before they could even get a diagnosis or wear they clothes they wanted. They also had to go to their employer and ask for a piece of paper, which was embarrassing. Access to healthcare was the start of the journey and would help people ‘be in the body they want to be in’.
Another had transitioned ten years ago and had only waited about 18 months for their first Gender Identity Clinic appointment, and that the waiting list was now about five years long. GPs should be able to prescribe hormones.
The CEO from Tonic Housing, a housing association set up specifically for LGBT+ people, told us that their retirement complex didn’t have any trans residents yet, but that the project had had the input of trans people throughout. Staff had received training from Opening Doors (who I note has a member of staff who I sat near at the last CliniQ conference, who demanded trans people be given jobs just because they are trans).
Then we learnt that someone had transitioned aged 16, buying medications over the internet because they had no access to gender identity services in their home country. They no longer wanted people to self-medicate and believed that GPs should be the prescribers. Ross told us that CliniQ supported people who self-medicate by providing advice on ‘how to do it safely’. Dr Brady said that local services should all join up together and also acknowledged that a sizeable contingent of people known to the service were self-sourcing hormones. No one said anything about the potential dangers of doing so, which clearly includes death if you end up eating rat poison.
Then a GP with a silly haircut introduced himself, and his pronouns, and that he was working closely with CliniQ on a project, but failed to specify exactly what, appearing to dry up. He also believed that GPs should manage hormone prescriptions and monitoring, and that admin and reception staff were key to making the difference.
Dr Brady said that trans people also have other healthcare needs, like sometimes they also got diabetes or broke their legs (again failing to mention the link between hormone use and bone health). Something needed to be done about GP databases.
16:10
Thank you’s.
Michelle Ross and Dr Michael Brady.
Summary
What an inspiring and thorough discussion. Repeatedly mooting the idea that GPs should carry the can for prescribing high dosages of cross sex hormones, especially to patients who may already have a complex set of clinical needs, is a complete waste of time since the Royal College of General Practitioners made a position statement on Transgender Care in June 2019. It is clear that they take a dim view of such demands.
GPs are facing increasing difficulties addressing patient requests for “bridging” prescriptions,
particularly for those patients who have self-started medication, including medication which
they have procured over the internet.GMC advice on ‘bridging prescriptions’ for trans and non-binary people recommends that
GPs should only consider issuing bridging prescriptions in cases where all the following criteria
are met:
a. the patient is already self-prescribing from an unregulated source (over the internet
or otherwise on the black market)
b. the bridging prescription is intended to mitigate a risk of self-harm or suicide, and
c. the doctor has sought the advice of an experienced gender specialist, and
prescribes the lowest acceptable dose in the circumstances.Additionally, GMC advice references a harm reduction approach, whereby GP or other
paragraph 24, Position statement from the RCGP
medical practitioners may prescribe bridging endocrine treatments as part of a holding or
harm reduction strategy while the patient awaits assessment and advice from a specialist, if it
is judged that this approach benefits the patient overall. However, this advice fails to address
the ethical and safety issues around prescribing outside the limits of one’s competence, the
significant medicolegal implications this carries and the non-pharmacological needs of patients
as they await access to a specialist.
The RCGP also say this about GnRH (puberty blockers) and other cross sex hormone treatment:
There is a significant lack of robust, comprehensive evidence around the outcomes, side effects and unintended consequences of such treatments for people with gender dysphoria, particularly children and young people, which prevents GPs from helping patients and their families in making an informed decision.
paragraph 15
Therefore, it is utterly pointless promoting the idea of GP taking on this responsibility nationally when this clear position statement is in existence and unchanged in almost three years. They need to read the statement and understand it. As for the constant harping on about clinic receptionists, only bullies focus their ire on the low paid.
Thank you for reading! Sign up to my blog by going to the bottom of the page.
Please share on other forums if you liked it, as I only do Twitter.

I was sent the 2021 GP Patient Survey and made a formal complaint about the gender ID question. I pointed out that they’d made it impossible to know who was which sex or even how many respondents actually considered themselves transgender as the separate questions were contradictory and self-cancelling. I got a useless, uncomprehending reply. It seems the NHS has rolled out this practice of refusing to ask straightforward Qs about biological sex. They can’t possibly even know how many trans-identified people responded as they totally screwed up collected such data.
LikeLiked by 2 people
It’s a real travesty. I think ultimately it probably isn’t that useful knowing how many people are trans-identified, but if you were going to do it you need to at least do it so that it is captured properly. It feels like they want to smash so much more than the ‘gender binary’.
LikeLiked by 1 person