
Yet again, the activists do a sterling job of ignoring health issues and detransitioners …

Introduction
Let’s face it, these are trying times for the gender identity cabal. The UK government is finally getting around to understanding that sex has meaning and should have in law. The whole debate about putting men in women’s prison has, care of ‘Isla Bryson‘, now happened more widely. But perhaps more than anything the gender industry has been damaged by the crescendo of voices speaking about medical malpractice they have suffered.
Introduction to the Day.
Michelle Ross Exec Director and Founder CliniQ What we do and why we do it. Ending Stigma Matters
This was CliniQ’s 9th annual conference, its first held in 2013. The restrictions of the pandemic had bought in a new mentoring system in which lives were ‘transformed’ and ‘saved’. Ross wanted to emphasise that Dr Michael Brady, National Advisor for LGBT Health, was very much an equal partner in the service. CliniQ had visited Bangkok to share and develop policy with colleagues there, which Ross believes could augment a big change internationally.
Keynote speech by Dr Ronx
Stigma, Impact on Health and Wellbeing for trans, non-binary and gender diverse people
Dr Ronx had laryngitis and wasn’t able to give their keynote speech. (Bitter disappointment doesn’t even begin to cover it.) They did, however, give participants the permission to lipread them and, funnily enough, was able to quite vigorously agitate later in the day.
Mpox what we need to know by Dr Michael Brady
What couldn’t you guess? The vast majority of those (high 90s) who had contracted the virus through sexual contact were ‘men who had had sex with men’. Lesions on genitals and in the rectum were a key symptom. About one-third were HIV positive and the virus was especially harmful to those whose HIV was poorly controlled. The name of the virus had been rebranded from Monkey Pox to the more chill-sounding MPox.
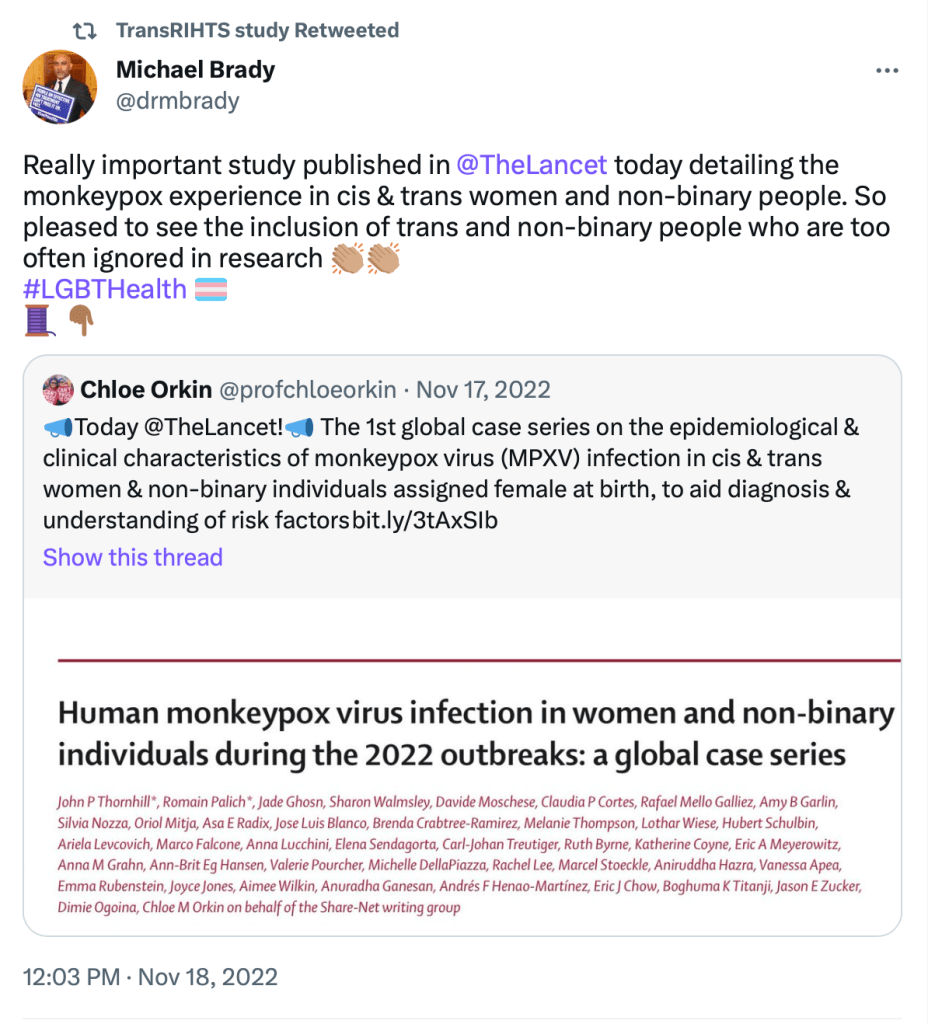
Brady spoke a bit about the paper (above) in which 62 trans-identified males, 69 women and five non-binary identified people (who were female) were studied. The non-binary persons data was combined, Brady explained, with the ‘cis women’ because it was too small a data set. Half of the trans-identified males who had contracted the virus were HIV positive in comparison to 8 percent of the females. Just like the main group studied, most had lesions on genitals with sexual transmission the likely route of infection (89 percent likelihood for males and 61 percent for females).
Over 70,000 people had received the first dose of the smallpox vaccine to safeguard against MPox, with around 27,000 having had the second. The vaccine programme was being wound down and he recommended that those in at risk groups get the vaccine, especially if they had advanced or uncontrolled HIV, as the mortality in that group was about 7 percent. And that, I think, was the only relevant piece of health advice we heard the whole day.
Ending HIV Stigma for trans and non-binary people
A time for change. Matthew Hodson, Exec Director NAM (Aidsmap).
Hodson informed us that he had visited CliniQ at the time it first opened to understand more about ‘transsexual health’ (interesting how taboo words are allowed when used by one of the anointed). Hodson became emotional explaining that his life was changed for the better after he gained trans friends, benefitting from their wisdom. He hated the ‘lies and nonsense’ about trans people currently being peddled (without mentioning what these might be). He also told us that HIV positive people have exactly the same longevity as those who don’t (which surely can’t be known yet, since retrovirals have only been in use for about forty years). It was important to understand the cumulative impact of intersectionality, e.g. a disabled black trans-identified male sex worker would have the most obstacles.
However, we did know that trans people were more likely to have mental health issues and that trans-led services would be more likely to understand ‘trans bodies’. His final faltering utterance, caused by a lump to his throat, was about standing with the community. Some murmured aah and Hodson got a very big round of applause for being a brave and stunning boy.
Christina Ansell, CEO Wandsworth Oasis (HIV charity)
Ansell was on hand to do a bit of trans awareness training needed by literally no one in the room. Ansell is concerned because most LGBTQI+ charities focus too much on the LGB, and not enough on the TQI+. Workplaces should allow the person ‘transitioning’ to take things at their own pace, allow ‘fuss free name changes’ and ask no questions about why they’re having time off. Make sure trans people are included across all policy areas, including things like parental leave, but especially have one which specifically covers trans healthcare. Ansell was ‘not going to mention toilets’ but did warn that people should be hyper-vigilant about micro-aggressions. When a newly transitioned person returns to work make sure you welcome them back by baking a cake or summink, because it takes a huge amount of courage to walk back through that door.
Victoria Cordoba, CliniQ Mentor, assessor, trainer.
Gave a brave and stunning talk about his journey from being a CliniQ patient to now director of the service. Not inappropriate at all, right?
Eli from Positively UK
Eli is a trans-identified female who is also HIV positive and currently works for a youth project. She described her experience of being HIV positive and trans as ‘liberating, isolating and exhausting’. She was interrupted several times by the organisers talking over her. Her sob story included the GP explaining they would only prescribe testosterone to her if it didn’t interfere with her HIV condition (some gasps in room). Eli had had to deal with both transphobia and the stigma of HIV, and a lack of compatriots in the same situation. I believe she said she had worked on a camp which supported HIV positive kids aged 11-16. She was asked a question about pregnancy guidelines for trans men with HIV and thought there was one in the making but couldn’t remember any details.
PrEP Matters for trans, non-binary and gender diverse people
Simon Collins Co-Founder i-Base (treatment activist group for HIV).
Collins said there was very little data on trans people with regards to PrEP use but also claimed that it was just as safe as for ‘cis people’. What he really meant to suggest is that people who are on cross sex hormones have no additional clinical problems, which seems unlikely when the same can cause hugely deranged liver and kidney function.
Activist Collins shares an office with Michelle Ross, Executive Director of CliniQ. i-Base refers to vaginal sex also as ‘front hole/frontal sex’.

General discussion
Dr Max Kelen, local GP, wondered how we could get more ‘cis women’ on PrEP. A commissioner in attendance said he was limited in what he could do to get PrEP out of level 3 and into the community and asked the assembled (mostly sexual health) professionals to ‘push harder please’. Collins wanted it to be available over-the-counter. A lone voice mentioned that patients on PrEP needed to let their GP know if they were on it so that renal function could be monitored. Another wanted PrEP to be available in the primary care setting. Then, finally, a trans-identified female said she didn’t want her GP to know that she was on PrEP, so hadn’t told her.

Josh Wells, Senior Clinical lead at LVNDR was in attendance at the meeting
There was very little awareness amongst pharmacists that trans people were sourcing cross sex hormones online.
GUMCAD and inclusive datasets, presentation by the UK Health Security Agency
It was time again for there to be quite a bit of talking over the speaker, the first of whom literally had the mic taken away from her and then unceremoniously shoved back into her face when it was deemed it had been fixed. The data was not for public release yet but the second speaker described the table that she was looking at in great detail. The bare bones of the matter is that when people visit Genitourinary Medicine (GUM) clinics they are now asked what their gender at birth is.
Can you spot the mistake?:

https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1032954/GUMCAD_starter_pack_2021.pdf
The statistics were to be released in the annual report but it was admitted there were problems with data completeness and that only two-thirds of the new dataset had included the question about gender at birth. If I noted correctly there were about 12,000 visits to GUM clinics made by trans/non-binary people (out of five million visits) of which around one-third were trans-identified female, half trans-identified males and the rest were ‘gender diverse’. These were mostly under the age of 25 and mostly seen face to face.
Studies; Hormone Levels Blood Test:
What they are for and why we do them
With Noeleen Bennett and Devon Buchanan from the TransRIHTs Study.

I don’t know why but I actually thought this was going to be a genuine item looking at the clinical protocols around managing people on cross sex hormones.
So, the study is being conducted by Kings College Hospital and sponsored by Synnovis (the UK laboratory, not to be confused with Synovis the US medical device manufacturer). RIHT stands for Reference Intervals while on Hormone Therapy Study. I think they should have just gone the whole hog and added in a G for Gender, as it really couldn’t sound more stupid. Or obvious.
Devon Buchanan introduced himself as she/they and is – apparently – a bona fide clinical data scientist who works for Synnovis. Buchanan put forward the scenario of non-binary person who had been on testosterone for five years and was tired all the time, so the GP measures the ferritin and the concentration comes back as 25mg/L. Buchanan said the normal range for males is 40-300mg/L for males and for females it is 20-200mg/L (Mr Google disagreed, but I have no idea), but was 25mg/L high or low for a non-binary person on testosterone? Which range should the GP refer to?
Well, first of all, Buchanan, non-binary is a completely made up identity which has no relation to the real world. So that’s the answer for you, provided by me, free of charge, so stand down. Fucking twat.
Buchanan’s mission was to make trans people feel less scary and unknowable to GPs. Buchanan let us know if patients weren’t on hormone therapy it was ‘quite likely’ their blood results would be in the same range as their sex assigned at birth. No shit.
So far they had recruited 166 participants to the meaningless study and wanted to get up to 240. Buchanan was keen to get the study over and done so that he could get his ‘life back’ (166 patients over 18 months, must have been rushed off his feet). Participants visit the CliniQ clinic on a Tuesday evening (so I guess another way of getting people in through the door with the promise of travel reimbursement). A questionnaire, bloods and urine samples were taken. The results weren’t ready yet and he wasn’t allowed to share any previews.
Ultimately Buchanan wanted labs to produce what the normal ranges for males and females on cross sex hormones should be onto patient results for trans people but he didn’t want to mention that. It seems a futile project, especially since so many use products bought from the web and therefore no one can know what dosages are being used, or the exact substances. As I understand it, even dosages prescribed in a clinical setting can be quite arbitrary, so that is one too many unstable factors.
Dr Ronx explained that she works as an emergency doctor at Homerton Hospital and was annoyed that the A&E service there recorded people as either male or female, leaving non-binary people out in the cold.
Buchanan tried to soothe Dr Ronx with the news that Kings College Hospital would be introducing a new Electronic Patient Record which would allow gender identity to be recorded. Dr Ronx still wailed that no one wanted to listen to her. I’m not sure what she expected Buchanan to do about it.
Contraceptive needs for trans men, non-binary people survey, with Dr Shruti Batham
Dr Batham claimed that there were high rates of unintended pregnancies amongst ‘trans and non-binary people’ (aka women). This was due to multiple barriers accessing contraception and lack of awareness of how to use it effectively. There was also the issue of testosterone use and users believing that it provided protection against pregnancy. She explained that the survey results were reviewed and validated by trans people (aka activists). The data was collected from paper surveys and online and that the results had been peer reviewed. Dr Batham threw the word ‘analysis’ around a lot.
Out of the 100 female participants, 72 identified as trans men, 14 were non-binary and genderqueer, and 14 ‘identified as both’. Racially 76 percent identified as white and the commonest age group was, incredibly, 35-44 years of age (unless I noted wrongly, which is always possible, if not, it shows that there is a definitive trend of older women transitioning). Dr Batham didn’t comment on the fact that pregnancy would be much less likely for this age group even in normal circumstances.
Most of the participants came from the South East/London area, most were on testosterone and that the mean time on that was three years. No one was taking hormone blockers (i.e. GnRH agonists). There was a mix of those who had purchased hormones through the internet and those who had a prescription via a gender identity clinic.
Of those on testosterone, Dr Batham said that the study showed 88 to 94 percent had understood the risks and side effects of being on the treatment. However, just 50 percent of the women had been counselled on the correct use of contraception. Similarly they had not been informed that testosterone would cause damage to a baby in utero. (Which makes a mockery of the suggestion that 88-94 percent had in fact understood the risks.)
Of the women who were actively engaged in sex with men very few were actively using any form of contraception. This was because there was a worry that contraception would make the exogenous testosterone less effective (presumably she meant the oral contraceptive pill, which contains a small dose of oestrogen).
Of the cohort there were seven unplanned pregnancies, of which three resulted in miscarriage, three in abortion and one which progressed to term. Four of these women were under 18.
In summary, 82 percent were not using any contraception (though I don’t think it was clarified what percentage were sleeping with men, I’m assuming most are, in fact, lesbians), 79 percent were on testosterone, of those only 50 percent had been counselled on the use of contraception before starting testosterone, and only 16 percent were referred on for further contraception advice. Five percent had used emergency contraception in the last year.
All of this proved that there needed to be a specialist service that fulfilled the needs of women who were trans-identified, though the more correct conclusion should have been that the study had simply proved that the gender identity pathway had failed to provide the correct care in the first place.
Dr Batham finished thanking Dr Michael Brady, her mentor and educational supervisor, who had been there every step of the way supporting her to complete this study and was responsible for the descriptive and thematic analysis (whatever that means). The paper will be published in due course.
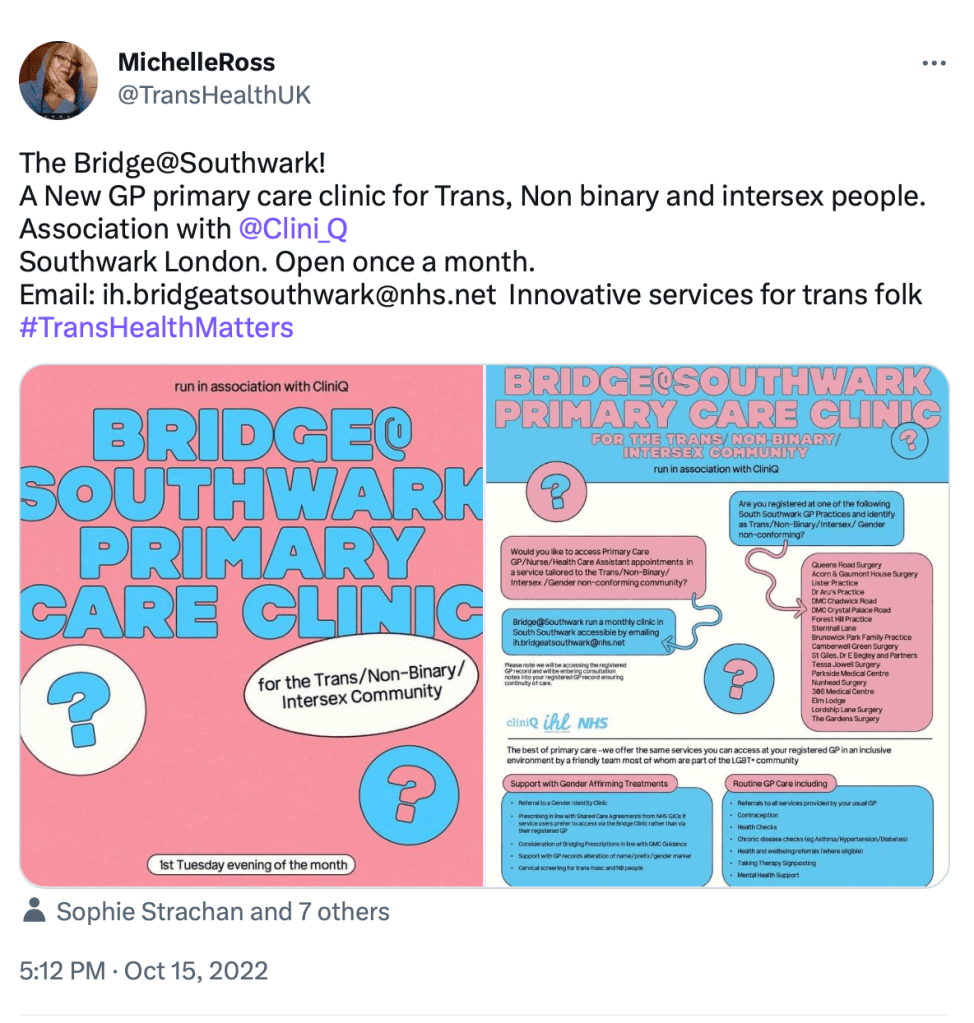
The First London GP service for Trans, Non-Binary and Gender Diverse People – Bridge At Southwark
Dr Rebecca Stephens, Flora Cohen senior nurse and Dr Max Kelen happen to be good friends who decided to set up a new service just for trans-identified patients registered with GPs in the South Southwark area.
Dr Rebecca Stephens
Dr Stephens has a practice in the same area and has provided a good chunk of the referrals for the new service. Interestingly, according to her blurb, she ‘especially enjoys seeing children and adolescents’ and holds a Diploma in Child Health and Obstetrics and Gynaecology, so you’d think she’d know better. Dr Stephens wore a rainbow skirt specially for the occasion and it sounded somewhat as if she had had one-on-one trans awareness training before arriving at the conclusion that cross sex hormones need to be prescribed and pushed onto, well, anyone who asks for them.

She casually informed us that as long as a GP had referred a patient to a Gender Identity Clinic there was absolutely no reason why they shouldn’t be prescribing hormones and claimed that hormones resolved gender dysphoria in most (but not all) patients.
(Which is interesting because a study written up by clinicians at the Gender Identity Clinic at the Tavistock and the UCL Institute of Child Health found there were no changes:
There were no changes from baseline to 12 or 24 months in CBCL or YSR total t-scores or for CBCL or YSR self-harm indices, nor for CBCL total t-score or self-harm index at 36 months. paragraph from Short-term outcomes of pubertal suppression in a selected cohort of 12 to 15 year old young people with persistent gender dysphoria in the UK, link to full article
The report avoids analysing girls and boys separately, as the preliminary results (for 30 out of 44 patients) were worse for girls. The report also documents that bone mineral loss is real and one can only wonder what the psychological impact of that must be on the patient cohort.)
Dr Stephens said that GICs didn’t have a contract to make these prescriptions but GPs did and gave a checklist of criteria:
- Make diagnosis of gender dysphoria.
- Take a history.
- Check consent – the patient must understand that the drugs will make permanent changes to their body.
- Mental health issues must be fairly well controlled.
- Must be aged over 17.
- Refer for gamete storage.
- Refer to Gender Identity Clinic.
Simples!
Dr Stephens also recommended Ben Vincent’s Transgender Health: A Practitioner’s Guide to Binary and Non-Binary Trans Patient Care. (Batshit Vincent has previously been a speaker at the CliniQ conference.)
Frankly Dr Stephens terrified me. A middle-aged woman whose midlife crisis appears to be to sterilise mentally compromised young adults. She was particularly proud that she had referred someone for gamete storage which had been accepted without question. Though it appeared it that had been on the basis that the patient was starting chemotherapy drugs, which is a bit of a lie, isn’t it? Moreover though I wondered what use she would be if one of her patients, new or old, came to her to explain that they had been the victim of medical malpractice. I expect her GP surgery probably wouldn’t be a safe space for that particular presentation, or provide a kind ear to a parent who didn’t want their teen to go on a pathway to permanent sexual dysfunction.
Flora Cohen
Cohen is another one clearly out of her depth. She cheerily informed us that she had found new two patients at the pub the previous week, at which people laughed. She was responsible for triaging the service by email (that’s after she’s bought them a drink at the bar presumably). Very giggly, Cohen kept making jokey comments to Dr Kelen sat by her side, as if she were a 14 year old, rather than a 30, possibly 40-something. The service provided all primary care services but their main drag were hormone prescriptions. No surprises there. Flora giggled a lot also that Dr Stephens is very much the one who sorted things out. Again, no surprises.
Dr Max Kelen
Dr Kelen, who I suspect is a trans-identified female, and, if so, therefore a user of testosterone, is also a specialist in sexual health and gynae issues. He updated us on the stats. The service had seen 30 new patients, of which roughly half were of the male gender and half female (presumably self-identified gender) and 91 percent were white, much to Dr Ronx’s great consternation but conversely great delight at the chance of rasping into a mega box sized microphone for what felt like the umpteenth time. Eighteen out of the 30 new patients had gotten brand new hormone prescriptions. One referral for ‘top surgery’ was made.
Someone in the audience made a joke about getting doctors to sign a prescription they hadn’t read and, again, people thought this was funny because getting on cross hormones is so anti-establishment doncha know.
I hope all three get sued.
Older Trans People Matter – Inclusive Care
In order to convince themselves that there is longevity in the cross sex hormone and butchery business, it was entirely fitting for this propaganda fest to end with the suggestion that a long life looms ahead. Though there were some fairly gloomy worries. About misgendering.

The elephant in the room
Yet again the assembled health professionals and activists failed to discuss anything of actual relevance to the health of those who are pursuing extreme body modification in the name of being ‘trans’. I’m always hopeful that there will be some adults in the room but the ideology cannot bear even the slightest scrutiny and hence we got nothing. Zero reflection on the known side effects of the drugs but worst of all zero mention of the growing number of men and women who testify that there were too young, now hate the situation they’re left in, and who have sustained irreversible damage.






But there is hope on the horizon – see here (‘Medical evidence over trans ideology: welcome to the doctors’ resistance’).
Thank you for reading! Sign up to my blog by going to the bottom of the page.
Please share on other forums if you liked it, as I only do Twitter.

You must be logged in to post a comment.